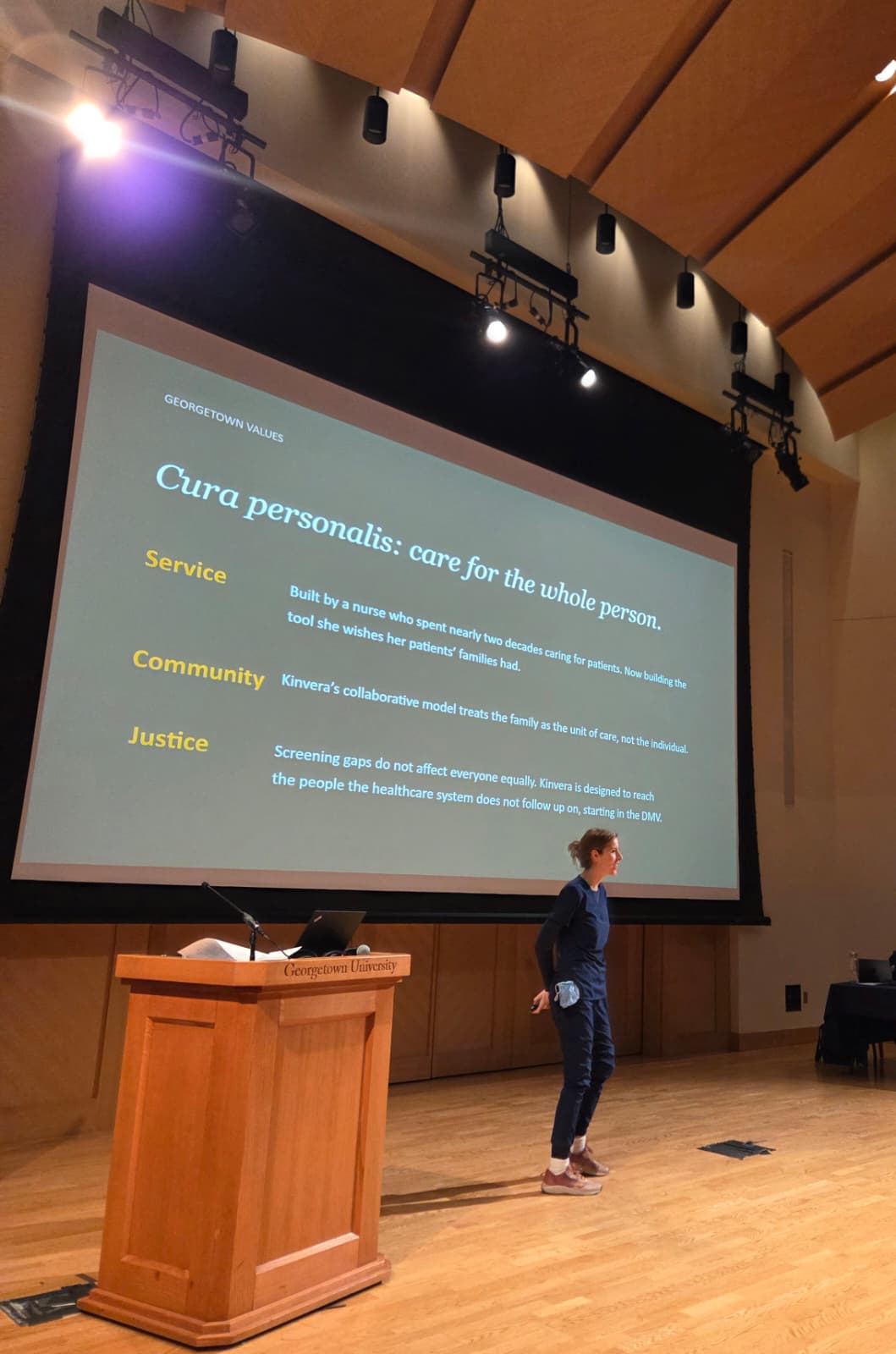
Why I built this.
Kinvera started in the ICU. Over years of critical care nursing, I watched the same scene play out at every bedside. A patient was in crisis. Their family was scrambling to fill in a history nobody had ever sat down to write. Sometimes nobody knew which side a condition came from. Sometimes the year of a diagnosis was a guess. It was always more chaotic than it needed to be, and the people who needed the information most were the ones who could not get it in the moment. The information almost always existed somewhere. It just had never been written down in one place.
The pattern was hard to miss once I started looking for it. We screen for the things we know to screen for, and we catch the things our doctors think to ask about. Family history, the single strongest predictor of inherited disease risk, was the part of the intake form that everyone filled out from memory, in five minutes, in a paper gown, the year of every diagnosis a rough guess.
So I built it for my own family first. We are spread across Maryland, California, Utah, Florida, and New Jersey. None of us could have told you, off the top of our heads, what conditions ran on which side. We had pieces. My mother knew her mother's history. My father knew his. Nobody had ever put it together into one document any of us could actually use.
Once I had a working version, I started asking other families if they wanted one. Every single person said yes. Nobody refused, and nobody told me they already had this handled. That is when I knew Kinvera was not a niche product for clinically-curious people. It was a layer of preventive care that the entire system has been skipping.
The version of this product I would have wanted, ten years ago, the first time I helped a family fill out a code status form while their parent was dying, is the version I am building now.